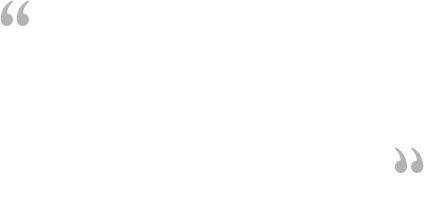
Age-related macular degeneration (AMD) is a degeneration or breakdown of the eye's macula. The macula is a small area in the retina (the light-sensitive tissue lining the back of the eye). The macula is the part of the retina that is responsible for your central vision, allowing you to read and see fine details clearly.
Even though the macula is only a small part of the retina, it is more sensitive to detail than the rest of the retina. The macula is what allows you to thread a needle, read small print, and recognize faces. The peripheral retina gives you side (or peripheral) vision.
If someone is standing to one side of your vision, your peripheral retina helps you know that person is there by allowing you to see their general shape. It is your macula that allows you to recognize the details of the person's face.
Many older people develop macular degeneration as part of the body's natural aging process. It is commonly called is age-related macular degeneration.
The retina is made up of many layers that work together to help you see clearly. AMD develops when a layer under the retina called the retinal pigment epithelium (RPE) is affected by deposits of tiny yellow or white pieces of fatty protein called drusens.
With AMD, you may have blurriness, dark areas or distortion in your central vision, and perhaps permanent loss of your central vision. It usually does not affect your side, or peripheral vision. For example, with advanced AMD, you could see the outline of a clock, yet may not be able to see the hands of the clock to tell what time it is.
Because the peripheral retina is spared, AMD alone almost never causes total blindness. People with more advanced cases of AMD continue to have useful vision using their side, or peripheral vision. When AMD does lead to loss of vision, it usually begins in just one eye, though it may affect the other eye later.
Many people are not aware that they have macular degeneration until they have a noticeable vision problem or until it is detected during an eye examination.
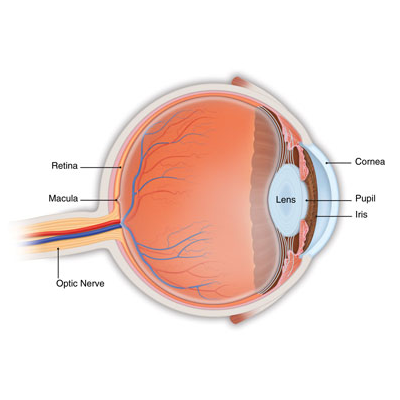
Photo of Normal Retina
There are two types of AMD:
1. Dry, or atrophic, AMD (also called non-neovascular AMD)
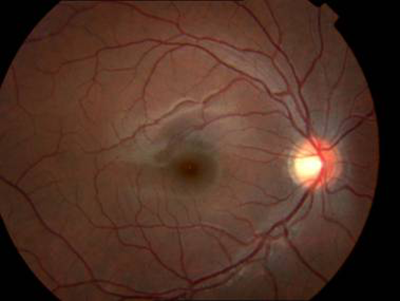
Most people who have AMD have the dry form. This condition is caused by aging and thinning of the tissues of the macula. Macular degeneration usually begins when tiny yellow or white pieces of fatty protein form under the retina (drusen). Eventually, the macula may become thinner and stop working properly. With dry AMD, vision loss is usually gradual.
Photo of Drusen
Monitoring your vision
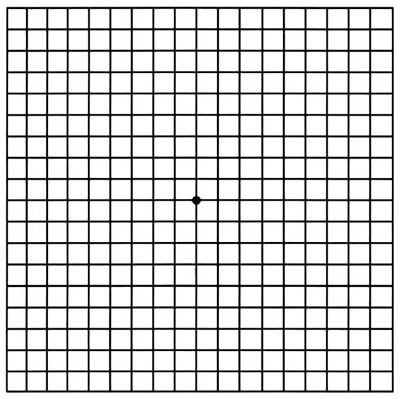
If you have been diagnosed with dry AMD, you should use a chart called an Amsler grid every day to monitor your vision, as dry AMD can change into the more damaging wet form. MEH provides Amslers charts for home use.
To use the Amsler grid, wear your reading glasses and hold the grid 12 to 15 inches away from your face in good light. Cover one eye.
Look directly at the center dot with the uncovered eye and keep your eye focused on it.
While looking directly at the center dot, note whether all lines of the grid are straight or if any areas are distorted, blurry or dark.
Repeat this procedure with the other eye.
If any area of the grid looks wavy, blurred or dark, contact your ophthalmologist immediately.
2. Wet, or exudative, AMD (also called neovascular AMD)
The wet form of macular degeneration occurs in only about 10 percent of all macular degeneration cases, but it can cause more damage to your central or detail vision than the dry form.
Capillaries, or tiny blood vessels, extend into all tissues of the body, bringing in nutrients and carrying off waste products. Capillaries usually don't increase in size or number, but if they do, it is called abnormal blood vessel growth.
An Amsler Chart:
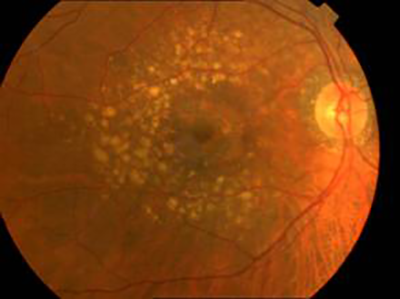
Photo of Wet AMD
Wet AMD occurs when abnormal blood vessels begin to grow underneath the retina. This blood vessel growth is called choroidal neovascularization (CNV) because these vessels grow from the layer under the retina called the choroid. These new blood vessels may leak fluid or blood, blurring or distorting central vision causing visual loss more noticeable than that from dry AMD.
The longer these abnormal vessels leak or grow, the more risk you have of losing more of your detailed vision. Also, if abnormal blood vessel growth happens in one eye, there is a risk that it will occur in the other eye. The earlier that wet AMD is diagnosed, the better chance you have of preserving some or much of your central vision. That is why it is so important that you and your ophthalmologist monitor your vision in each eye carefully.
What are the symptoms of AMD?
In its earliest stages, macular degeneration may cause the following symptoms:
Blurry distance and/or reading vision.
Distorted vision - straight lines will appear bent, crooked or irregular.
Dark gray spots or blank spots in your vision.
Size of objects may appear different for each eye.
Colors do not look the same depth / brightness for each eye.
What causes AMD?
The exact cause of AMD is not known, but it is clear that this disease is strongly associated with age, since AMD occurs as people grow older. One large study found that the risk of getting AMD jumps from about 2 percent of middle-aged people in their 50s to nearly 30 percent in people over age 75.
Our bodies constantly react with the oxygen in our environment. Over our lifetimes, as a result of this activity, our bodies produce tiny molecules called free radicals. These free radicals affect our cells, sometimes damaging them. This is called oxidative stress and is thought to play a major role in how AMD develops.
Heredity is another risk factor for AMD. People who have a close relative with the disease have a greater chance of developing AMD themselves.
Some studies have shown that inflammation (swelling of the body's tissues) may play a role in AMD development. Inflammation is the way the body's immune system fights off infection or other things it considers "invaders." But an overactive immune system with its associated inflammation may be a risk factor for AMD.
Smoking and high blood pressure are associated with the wet form of AMD. Research also suggests there may be a link between being obese and having AMD.
Who is at risk for AMD?
Major risk factors for AMD are:
Being older than 50 years old.
Having a family history of AMD.
Cigarette smoking.
Another risk factor for developing AMD may include having abnormal cholesterol levels or having high blood pressure (hypertension).
How is AMD diagnosed?
Many people do not realize they have a macular problem until they notice they have blurred or distorted vision. Regular eye examinations by an ophthalmologist may help to detect problems before you are even aware of them. Your ophthalmologist can see early stages of AMD during a comprehensive eye examination.
The American Academy of Ophthalmology recommends that adults with signs or risk factors for eye disease get a baseline eye disease screening at age 40 - the time when early signs of disease and changes in vision may start to occur. Based on the results of the initial screening, an ophthalmologist will prescribe the necessary intervals for follow-up exams.
To check for macular degeneration, your eye doctor will dilate (widen) your pupils using eye drops and examine your eyes with an ophthalmoscope or 90 D lens that allows him or her to see the retina and other areas at the back of the eye. If AMD is detected, your doctor may have you use an Amsler grid to check for wavy, blurry or dark areas in your vision.
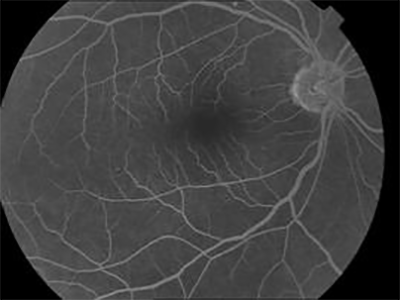
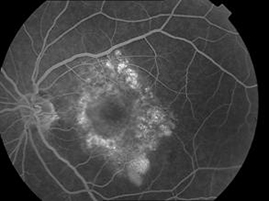
Fluorescein angiography
If your ophthalmologist finds an abnormality during an exam and suspects the wet form of AMD, he or she will take special photographs of your eye called fluorescein angiography (FFA). These photographs determine if abnormal blood vessels are under the retina.
To do this test, fluorescein dye is injected into a vein in your arm. The dye travels throughout the body, including your eyes. Photographs are taken of your eye as the dye passes through the retinal blood vessels. Abnormal areas will be highlighted by the dye, indicating to your doctor whether treatment is possible.
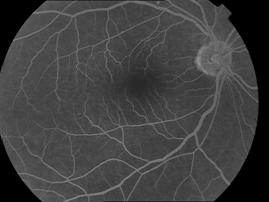
Normal FFA
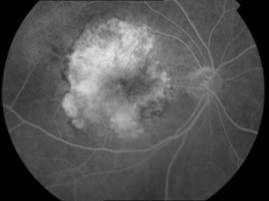
FFA of AMD
If treatment options are available, these photographs will provide your doctor with a map to guide the treatment
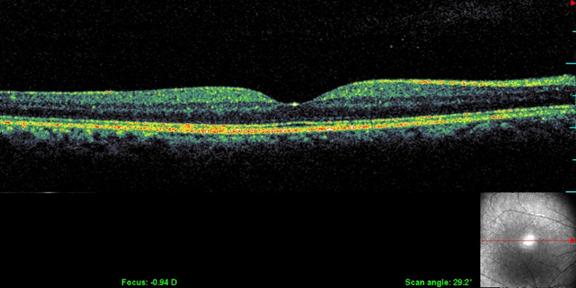
Optical Coherence Tomography (OCT)
OCT is a non-radiation mode of scanning that utilizes certain light waves for the scan.
OCT can show the retinal layers almost as if in biopsy (layer by layer). The resolution of the Spectral OCT scan available in MEH is 5 microns. Such highly precise scans help your doctor diagnose your AMD quite effortlessly.
Normal OCT
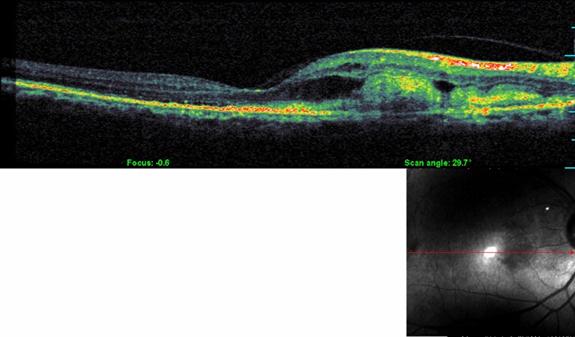
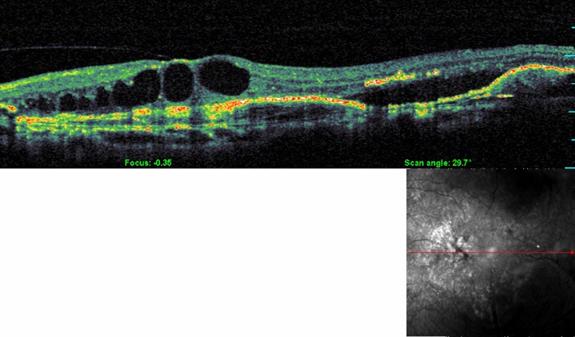
OCT in AMD
OCT is the most sensitive scan for monitoring the progress of AMD as well as for assessing the response to treatment.
How is AMD treated?
Unfortunately, at this time there is no single proven treatment for the dry form of AMD. However, a large scientific study has shown that antioxidant vitamins and zinc may reduce the impact of AMD in some people by slowing its progression toward more advanced stages.
The Age-Related Eye Disease Study (AREDS) showed that among people at high risk for developing late-stage, or wet, AMD (such as those who have large amounts of drusen or who have significant vision loss in at least one eye), taking a dietary supplement of vitamin C, vitamin E and beta carotene, along with zinc, lowered the risk of AMD progressing to advanced stages by about 25 percent. The daily supplements also reduced the risk of vision loss for those at risk by about 19 percent. The AREDS nutrient supplementation shown to be beneficial includes:
Vitamin C - 500 mg
Vitamin E - 400 IU
Beta carotene - 15 mg (25,000 IU)
Zinc oxide - 80 mg
Copper (as cupric oxide) - 2 mg (to prevent copper deficiency, which may be associated with taking high amounts of zinc)
Another large study in women showed a benefit from taking folic acid and vitamins B6 and B12. And a large study evaluating the possible benefits of lutein and fish oil (omega-3) is ongoing.
It is very important to remember that vitamin supplements are not a cure for AMD, nor will they give you back vision that you may have already lost from the disease. However, specific amounts of these supplements do play a key role in helping some people at high risk for developing advanced (wet) AMD to maintain their vision. Talk with your ophthalmologist to find out if you are at risk for developing advanced AMD, and to learn if supplements are recommended for you.
Treating wet AMD
UTreating the wet form of AMD may involve the use of anti-VEGF treatment, thermal laser treatment or photodynamic therapy (PDT). Treatment of wet AMD generally reduces the risk of severe vision loss, but it does not eliminate this risk.
Anti-VEGF treatment
A common way to treat wet AMD targets a specific chemical in your body that causes abnormal blood vessels to grow under the retina. That chemical is called vascular endothelial growth factor, or VEGF. Several new drugs (called anti-VEGF drugs) have been developed that can block the trouble-causing VEGF. Blocking VEGF reduces the growth of abnormal blood vessels, slows their leakage, helps to slow vision loss, and in some cases improves vision.
Your ophthalmologist administers the anti-VEGF drug directly to your eye as an injection. Before the procedure, your ophthalmologist will clean your eye to prevent infection and will use an anesthetic to numb your eye with a very fine needle. You may have to receive multiple anti-VEGF injections over the course of many months.
In some cases, your ophthalmologist may recommend combining anti-VEGF treatment with other therapies. The treatment that's right for you will depend on the specific condition of your macular degeneration. Currently available anti-VEGFs are Avastin and Lucentis.
Thermal laser treatment
Another form of treatment for wet AMD is with thermal laser therapy. Laser treatment is usually done as an outpatient procedure in MEH.
The laser beam in this procedure is a high-energy, focused beam of light that produces a small burn when it hits the area of the retina to be treated. This destroys the abnormal blood vessels, preventing further leakage, bleeding and growth.
Following laser treatment, vision may be more blurred than before treatment, but often it will stabilize within a few weeks. A scar forms where the treatment occurred, creating a permanent blind spot that might be noticeable in your field of vision.
Usually the abnormal blood vessels are destroyed by laser treatment. However, it is likely that 50 percent of patients with wet AMD who receive this laser procedure will need a re-treatment within three to five years. You may be instructed to use the Amsler grid daily to monitor your vision for signs of change.
Photodynamic therapy (PDT)
In some cases, a type of treatment for wet AMD called photodynamic therapy, or PDT, may be an option.
This therapeutic procedure uses a combination of a light-activated drug called a photosensitizer and a special low-power, or cool, laser to treat wet AMD right at the center of the macula. This procedure is done on an outpatient basis. The photosensitive drug is injected into a vein in your arm, where it travels through the body, including the abnormal vessels behind the central macula. The low-power laser light is targeted directly on the abnormal vessels, activating the drug, which causes damage specifically to those unwanted blood vessels.
Multiple treatments may be required.
What happens when AMD cannot be treated?
It is important to remember that only about 10 percent of all AMD cases are exudative, or wet form, and about 75 percent of these cases cannot be treated. People with wet or dry AMD who cannot be treated will not become blind, as they will still have peripheral, or side, vision.
If you have untreatable AMD, you can make the most of your remaining vision by learning to "see again" with the vision you do have and with the help of special low-vision rehabilitation, devices and services.
While there is little that can be done to improve the eyesight of someone who has AMD, with early detection, the rate of vision loss can be slowed. The keys to slowing vision loss are to understand your condition and work closely with your ophthalmologist to monitor your vision. Even with macular degeneration, you can still maintain an enjoyable lifestyle.
Low-vision aids
There are many devices specifically designed to help people with low vision function better. Different devices are available for different tasks. A trained professional can help you understand which device is best for accomplishing your particular needs. Training and practice are also important in order to become skilled at using any device.
Optical low-vision devices.
Optical low-vision devices use lenses to magnify objects, making them easier to see. The lens strength will depend on your vision and the size of the object or print to be seen.
Magnifying spectacles. Stronger than ordinary glasses. They can be used for near tasks, such as reading, threading a needle, or any activity that requires detailed vision. The printed page or object must be held closer than usual in order to keep things in focus. One advantage of magnifying spectacles is that your hands remain free to hold reading materials or perform tasks.
Hand magnifiers. Familiar to most people and are available in varying strengths. Reading material is not necessarily held as close to the face as with magnifying spectacles, and some models come with a built-in light. High-quality and high-powered magnifiers are often available only in specialized stores or through vision rehabilitation professionals.
Stand magnifiers. Rest directly on the reading material, keeping the lens at the proper distance from the page. The ability to rest the magnifier on the page is useful for patients with a tremor or arthritis.
Telescopes. Used for seeing objects or reading signs that are far away. They can be handheld like a pair of regular binoculars or mounted on a pair of eyeglasses.
Video magnifiers. Electronic devices that use a camera and television screen to enlarge printed material, pictures, or small objects. They are adjustable and can enhance the material in different ways - for example, by making the print appear darker (increased contrast).
Other low-vision devices and techniques
There are numerous low vision aids, devices, and techniques to help make everyday activities easier. They include:
Large-print books, newspapers, magazines, etc.
Computers that can magnify any printed material or picture, or that read aloud what is viewed on screen.
Lighting and glare
Good lighting and glare control are very important for people with low vision. A bright light should always be used when reading and its location should be adjusted for the greatest visibility without glare.
Stronger light bulbs in darkly lit areas can make tasks like cooking, dressing, and walking up and down stairs easier. A tinted, wraparound sunglass can shield your eyes from dazzling and annoying overhead lights or sunlight.