Glaucoma is a disease that damages the eye's optic nerve. The optic nerve is made up of many nerve fibers, like an electric cable is made up of many wires. The optic nerve sends signals from your retina (a layer of light-sensitive tissue lining the back of the eye) to your brain, where these signals are interpreted as the images you see.
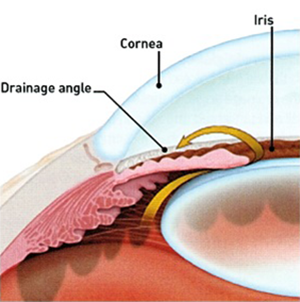
If the drainage angle is blocked, excess fluid cannot flow out of the eye, causing the fluid pressure to increase.
In the healthy eye, a clear fluid called aqueous humor circulates inside the front portion of your eye. To maintain a constant healthy eye pressure, your eye continually produces a small amount of aqueous humor while an equal amount of this fluid flows out of your eye.
The fluid flows out through a very tiny drain called the trabecular meshwork, a complex network of cells and tissue in an area called the drainage angle.
If you have glaucoma, the aqueous humor does not flow through the trabecular meshwork properly. Fluid pressure in the eye builds up and over time causes damage to the nerve fibers.
Glaucoma can cause blindness if it is left untreated.
When glaucoma develops, usually you don't have any early symptoms and the disease progresses slowly. That is why it is called "silent thief of sight". Fortunately, early detection and treatment can help preserve your vision.
There are several types of glaucoma:
Open-angle glaucoma
The most common form of glaucoma is called primary open-angle glaucoma. It occurs when the trabecular meshwork of the eye gradually becomes less efficient at draining fluid. As this happens, your eye pressure, called intraocular pressure (IOP), rises. Raised eye pressure leads to damage of the optic nerve. Damage to the optic nerve can occur at different eye pressures among different patients.
Typically, open-angle glaucoma has no symptoms in its early stages and vision remains normal. As the optic nerve becomes more damaged, blank spots begin to appear in your field of vision. You usually won't notice these blank spots in your day-to-day activities until the optic nerve is significantly damaged and these spots become large. If all of the optic nerve fibers die, the result will be blindness.
Half of patients with glaucoma do not have high eye pressure when first examined. That is why it is essential that the optic nerve be examined by an ophthalmologist for proper diagnosis.
Normal-tension glaucoma
Eye pressure is expressed in millimeters of mercury (mm Hg), the same unit of measurement used in weather barometers.
Although normal eye pressure is considered a measurement less than 21 mm Hg, this can be misleading. Some people have a type of glaucoma called normal-tension, or low-tension glaucoma. Their eye pressure is consistently below 21 mm Hg, but optic nerve damage and visual field loss still occur. People with normal-tension glaucoma typically receive the same methods of treatment used for open-angle glaucoma.
Conversely, ocular hypertension is a condition where someone has higher eye pressure than normal, but does not have other signs of glaucoma, such as optic nerve damage. Someone with ocular hypertension is considered a "glaucoma suspect" because he or she may be at risk for developing glaucoma later. Just like people with glaucoma, people with ocular hypertension need to be closely monitored by an ophthalmologist to ensure they receive appropriate treatment.
Closed-angle glaucoma
A less common form of glaucoma is closed-angle, or narrow-angle, glaucoma. Closed-angle glaucoma occurs when the drainage angle of the eye becomes blocked. Unlike open-angle glaucoma, eye pressure usually goes up very fast. The pressure rises because the iris - the colored part of the eye - partially or completely blocks off the drainage angle. People of Asian descent and those with hyperopia (farsightedness / long sight) tend to be more at risk for developing this form of glaucoma.
If the drainage angle becomes completely blocked, eye pressure rises quickly resulting in a closed-angle glaucoma attack. Symptoms of an attack include:
Severe eye or brow pain;
Redness of the eye;
Decreased or blurred vision;
Seeing colored rainbows or halos;
Headache;
Nausea;
Vomiting.
A closed-angle glaucoma attack is a medical emergency and must be treated immediately.
People at risk for closed-angle glaucoma should avoid over-the-counter decongestants (usually taken for common cold) and other medications contraindicated in glaucoma (mentioned in the drug packing / pamphlet).
Congenital glaucoma
Congenital glaucoma is a rare type of glaucoma that develops in infants and young children. It happens when the eye's drainage system doesn't develop fully or correctly before birth. Congenital glaucoma can be inherited
Secondary glaucoma
Glaucoma can often develop as the result of another eye condition or disease. This is known as secondary glaucoma. For example, someone who has a tumor or people undergoing long-term steroid therapy may develop secondary glaucoma. Other causes of secondary glaucoma include:
Eye injury
Inflammation of the eye
Abnormal blood vessel formation from diabetes or retinal blood vessel blockage;
Use of steroid-containing medications (pills, eye drops, sprays);
Pigment dispersion: tiny fragments or granules from the iris (the colored part of the eye) can circulate in the aqueous humor (the fluid within the front portion of the eye) and block the trabecular meshwork, the tiny drain for the eye's aqueous humor.
What are the symptoms of glaucoma?
In its early stages, glaucoma has no symptoms. As the disease progresses and more damage occurs, blind spots develop in your peripheral (side) vision. These spots may not be noticeable until the optic nerve has become severely damaged - or until detected by an ophthalmologist during a complete exam.
People at risk for closed-angle glaucoma, where the eye's drainage angle becomes blocked, usually have no symptoms before the attack, though some early symptoms can include blurred vision, halos, headache or mild eye pain or redness. At the time of a closed-angle glaucoma attack, symptoms include:
Severe eye or brow pain.
Redness of the eye.
Decreased or blurred vision.
Seeing colored rainbows or halos.
Headache
Nausea
Vomiting
People with "normal-tension glaucoma" may have eye pressures within normal ranges, but have glaucoma signs and symptoms, such as blind spots in their field of vision and optic nerve damage.
Some people may not have glaucoma symptoms, but may have higher than normal eye pressure (called ocular hypertension). They are considered "glaucoma suspects," and should be monitored carefully by an ophthalmologist.
Who is at risk for glaucoma?
Some people are at greater risk for developing glaucoma and should see their ophthalmologist on a regular basis, specifically for glaucoma testing. Risk factors for glaucoma include:
Age
Family history of glaucoma.
Farsightedness or nearsightedness.
Elevated eye pressure.
Past eye injury.
Having a thinner central cornea.
Not having eye examinations when they are recommended.
Conditions that affect blood flow, such as migraines, diabetes and low blood pressure.
How is glaucoma diagnosed?
One of the problems with glaucoma, especially open-angle glaucoma, is that there are typically no symptoms in the early stages. Many people who have the disease do not know they have it. This is why it is important, especially as you get older, to have regular medical eye exams by an ophthalmologist.
The eye examination
In a glaucoma evaluation, your doctor:
Measures the pressure in your eye (tonometry)
Inspects your eye's drainage angle (gonioscopy)
Inspects your optic nerve (ophthalmoscopy)
Tests your side, or peripheral, vision (visual field test / perimetry)
Measures the thickness of your cornea - the clear window at the front of the eye (pachymetry).
Tonometry exam
During this test, your eye is numbed with eyedrops. Your doctor uses an instrument called a tonometer to measure eye pressure. The instrument measures how your cornea resists pressure.
Normal eye pressure generally ranges between 10 and 21 mm Hg.
Gonioscopy exam
Gonioscopy allows your ophthalmologist to get a clear look at the drainage angle to determine the type of glaucoma you may have. By using a mirrored lens, your ophthalmologist can examine the drainage angle to determine if you have open-angle glaucoma (where the drainage angle is not working efficiently enough), closed-angle glaucoma (where the drainage angle is at least partially blocked), or a dangerously narrow angle (where the iris is so close to the eye's drain that the iris could block it).
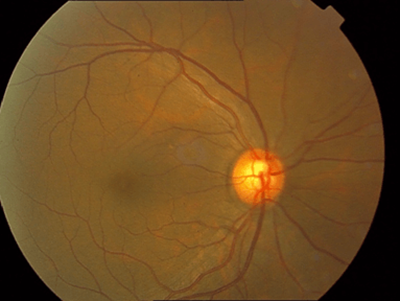
Ophthalmoscopy exam
Your ophthalmologist inspects your optic nerve for signs of damage using an ophthalmoscope or 90D lens. Your pupils might be dilated (widened) with eyedrops to allow your doctor a better view of your optic nerve.
Normal Optic Disc
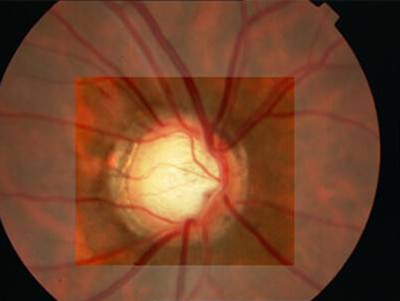
Glaucoma Cupping
A normal optic nerve is made up of more than one million tiny nerve fibers. As glaucoma damages the optic nerve, it causes the death of some of these nerve fibers. As a result, the appearance of the optic nerve changes. This is referred to as cupping. As the cupping increases, blank spots begin to develop in your field of vision.
Visual field test
The visual field test will check for blank spots in your vision. The results of the test show your ophthalmologist if and where blank spots appear in your field of vision - including spots you may not even notice.
The test is performed using a bowl-shaped instrument called a perimeter. When taking the test, a patch is temporarily placed on one of your eyes so that only one eye is tested at a time. You will be seated and asked to look straight ahead at a target. Random points of light will flash around the bowl-shaped perimeter, and you will be asked to press a button whenever you see a light. Visual field testing is usually performed every 6 to 8 months to monitor for change.
Pachymetry
Because the thickness of the cornea can affect eye pressure readings, pachymetry is used to measure corneal thickness. A probe called a pachymeter is gently placed on the cornea to measure its thickness.
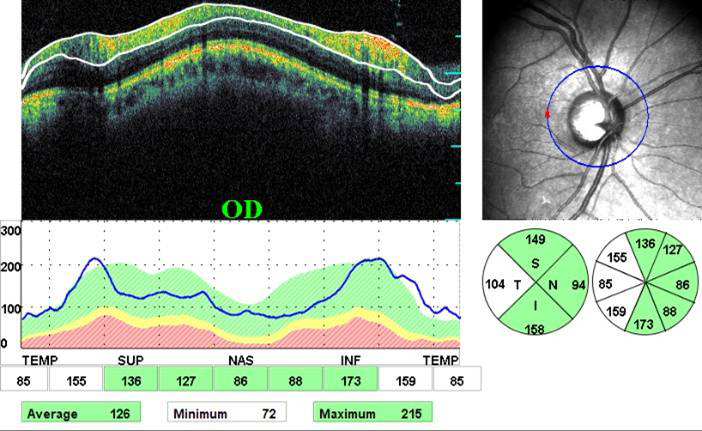
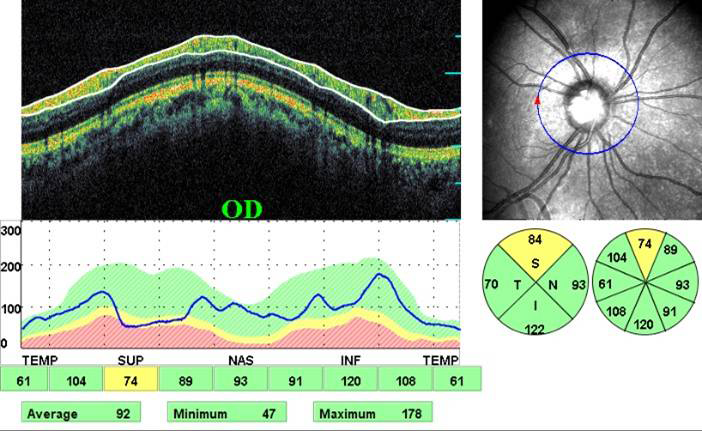
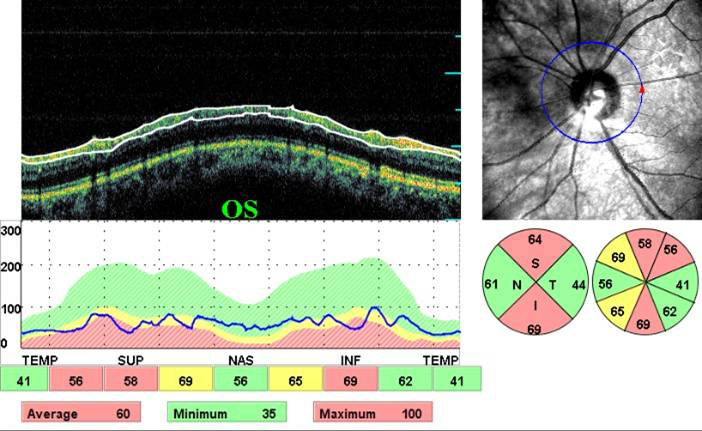
Optical Coherence Tomography (OCT)
OCT is a non-radiation mode of scanning that utilizes certain light waves for the scan.
OCT can show the tissue in detail almost as if in biopsy (layer by layer). The resolution of the Spectral OCT scan available in MEH is 5 microns. Such highly precise scans help your doctor diagnose your condition and monitor progress quite effortlessly.
OCT and RNFL Analysis
This is an optical scan that measures the thickness of the retinal nerve fiber layer immediate to the optic disc. A thin retinal nerve fiber layer (RNFL) points to glaucoma. OCT (Optical coherence tomography) can also be used for optic nerve analysis.
Normal OCT
Early Glaucoma Damage
Severe Glaucoma Damage
OCT and the Angle
OCT can be used to measure the angle of the eye (from where the aqueos fluid is supposed to drain out) and assess the likelihood of angle closure glaucoma. OCT can also be employed to verify whether the angle has opened up after laser treatment for glaucoma (ALT, SLT or YAG Iridotomy).
OCT and Pachymetry
OCT scan of the cornea provides a true optical measurement of the corneal thickness. This influences the choice of treatment and hence is a useful tool in glaucoma treatment.
Early detection and treatment can protect your vision.
People of any age with symptoms of or risk factors for glaucoma, such as those with diabetes, a family history of glaucoma, or those of African descent, should see an ophthalmologist for an exam. Your ophthalmologist will let you know how often to return for follow-up exams.
Adults with no symptoms of or risk factors for eye disease should have a complete eye disease screening by age 40 - the time when early signs of disease and changes in vision may start to happen. Based on the results of the initial screening, your ophthalmologist will let you know how often to return for follow-up exams.
Adults 65 or older should have an eye exam every one to two years, or as recommended by your ophthalmologist.
If you have glaucoma, preserving your vision requires strong teamwork between you and your doctor. Your doctor can prescribe treatment, but it's important to do your part by following your treatment plan closely. Be sure to take your medications as prescribed and see your ophthalmologist regularly.
How is glaucoma treated?
How your glaucoma is treated will depend on your specific type of glaucoma, the severity of your disease, and how it responds to treatment.
Medicine
Medicated eye drops are the most common way to treat glaucoma. These medications lower your eye pressure in one of two ways - either by slowing the production of aqueous humor or by improving the flow through the drainage angle.
These eye drops must be taken every day. Just like any other medication, it is important to take your eye drops regularly as prescribed by your ophthalmologist.
Never change or stop taking your medications without consulting your doctor.
Surgery
In some patients with glaucoma, surgery is recommended. Glaucoma surgery improves the flow of fluid out of the eye, resulting in lower eye pressure.
Laser trabeculoplasty
To treat open-angle glaucoma, a surgery called laser trabeculoplasty is often used. There are two types of trabeculoplasty surgery: argon laser trabeculoplasty (ALT) and selective laser trabeculoplasty (SLT).
During ALT surgery, a laser makes tiny, evenly spaced burns in the trabecular meshwork. The laser does not create new drainage holes, but rather stimulates the drain to function more efficiently.
SLT treats specific cells and leaves the mesh-like drainage canals surrounding the iris intact. SLT may be an alternative for those who have been treated unsuccessfully with traditional laser surgery or with pressure-lowering drops.
Even if laser trabeculoplasty is successful, most patients need to continue taking glaucoma medications. For many, this surgery is not a permanent solution. Nearly half who receive this surgery develop increased eye pressure again within five years and need to have a repeat treatment.
Laser iridotomy
Laser iridotomy is recommended for treating people with closed-angle glaucoma and those with very narrow drainage angles. A laser creates a small hole about the size of a pinhead through the top part of the iris to improve the flow of aqueous fluid to the drainage angle. This hole is hidden from view by the upper eyelid.
Trabeculectomy
In trabeculectomy, a small flap is made in the sclera (the outer white coating of your eye). A filtration bleb, or reservoir, is created under the conjunctiva - the thin, filmy membrane that covers the white part of your eye. Once created, the bleb looks like a blister on the white part of the eye above the iris, but the upper eyelid usually covers it. The aqueous humor can now drain through the flap made in the sclera and collect in the bleb, where the fluid will be absorbed into blood vessels around the eye.
During surgery, the scleral flap is closed with tiny stitches. Some of these stitches may be removed after surgery to increase drainage. Medication to reduce scarring is often used during and after surgery.
Eye pressure is effectively controlled in three out of four people who have trabeculectomy.
Important things to remember about glaucoma:
Vision loss from glaucoma usually can be prevented if it is detected and treated early enough.
If you use eye drops to treat glaucoma, be sure to continue taking the medication as your doctor tells you to. Never change or stop taking your medications without consulting your doctor.
There are a number of ways to treat glaucoma. While some people may experience side effects from medications or surgery, the risks of side effects should always be balanced with the greater risk of leaving glaucoma untreated and losing vision.